The key to learning Korean is how easy it is to stay motivated to learn the language. At TalkToMeInKorean.com, we provide a systematic curriculum of easy-to-follow lessons, and a wide selection of self-study Korean-learning books!
…
continue reading
Content provided by joel topf and Channel Your Enthusiasm. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by joel topf and Channel Your Enthusiasm or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://ro.player.fm/legal.
Similar cu Channel Your Enthusiasm
Interviews with mathematics education researchers about recent studies. Hosted by Samuel Otten, University of Missouri. www.mathedpodcast.com Produced by Fibre Studios
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
From host Kevin Miller: When I was 7 years old and got out of line, my parents would give me an “attitude adjustment” and make me listen to motivational speakers like Zig Ziglar. I didn’t appreciate it at the time but the experience gave me awareness of how powerful our minds and outlook on life are. I went on to become a pro athlete, have 9 kids, start 17 businesses and become addicted to performance and production. Till I burnt out. Multiple times. That started a quest to not just pursue p ...
…
continue reading
The award-winning Curiosity Daily podcast from CuriosityDaily.com will help you get smarter about the world around you. In less than 10 minutes, you’ll get a unique mix of research-based life hacks, the latest science and technology news, and more. Nate Bonham and Calli Gade will help you learn about your mind and body, outer space and the depths of the sea, and how history shaped the world into what it is today.Head to discovery+ to stream even more science content, from Animal Planet to Sc ...
…
continue reading
Emergency Medicine Cases – Where the Experts Keep You in the Know. For show notes, quizzes, videos and more learning tools please visit emergencymedicinecases.com
…
continue reading
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
The London School of Economics and Political Science public events podcast series is a platform for thought, ideas and lively debate where you can hear from some of the world's leading thinkers. Listen to more than 200 new episodes every year.
…
continue reading
Culips English Podcast: Practical English Learning Made Fun Learn and Explore: Join Culips for an exciting English learning journey. Our podcast focuses on teaching English idioms, slang, and phrasal verbs through fun and engaging conversations. Each episode helps you master English for real-life situations. Unique Learning Experience: Culips stands out by blending language skills with cultural insights. Our diverse hosts make learning relatable, covering a variety of everyday topics. You’ll ...
…
continue reading
Player FM - Aplicație Podcast
Treceți offline cu aplicația Player FM !
Treceți offline cu aplicația Player FM !

))
Chapter two part two
Manage episode 288581724 series 2867323
Content provided by joel topf and Channel Your Enthusiasm. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by joel topf and Channel Your Enthusiasm or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://ro.player.fm/legal.
The exciting conclusion to
Chapter Two: Renal Circulation and Glomerular Filtration Rate
- Determinants of GFR
- First step in making urine is separation of an ultrafiltrate
- Governed by starling forces
- Balance of hydraulic and osmotic forces
- GFR = LpS (P gc – P us - Osmotic Pressure Cap p)
- Normal GFR 95 in women, 120 in men
- Cap Hydrolic pressure remains constant
- glom cap Oncotic progressively rises
- Due to filtration of protein free fluid (protein concentration rises in the capillary)
- Filtration gradient begins at 13 mmHg and falls to zero after filtration of 20% or RPF!
- GFR is capped at 20% of RPF called filtration equilibrium
- So GFR is dependent on RPF, unless you can change glomerular hydraulic pressure
- Glomerular hydraulic pressure is controlled by balance of twin arteriole (afferent and efferent)
- Constriction of afferent arteriole reduces RPF, GFR, and glom pressure
- Dilation of afferent arteriole increases RPF, GFR, and glom pressure
- Constriction of the efferent arteriole increases Glom pressure, increasing GFR
- Besides glom hydrostatic pressure the other starlings forces are rarely relevant to changes in GFR
Letty says: referred to this NEJM review article later JC thought she was referring to something else -see #2- and then Roger referred to this again)
Normotensive Acute Renal Failure from Gary Abuelo in NEJM 2007. https://www.nejm.org/doi/10.1056/NEJMra064398 (note in this article, Dr. Abuelo acknowledges the newer terminology of the time, AKI rather than ARF but chooses not to embrace it). In figure 2, he highlights the classic examples of how autoregulation can be affected. In the table, additional examples are provided but all within the framework of alterations related to autoregulation and the interplay between the two resistance vessels.
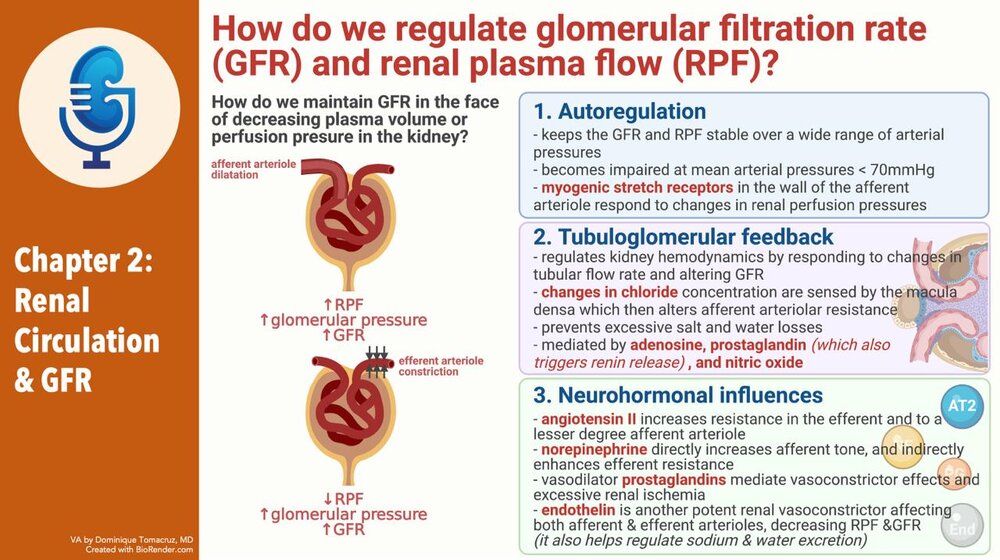
- Regulation of GFR
- Autoregulation
- The ability to keep glomerular pressure constant over wide range of systemic arterial pressure
- When pressure < 70 autoregulation fails and GFR will fall with decreases in systemic pressure
- When pressure falls below 40-50 GFR ceases
- At least some of this autoregulation is mediated with Ang2. Giving ACEi markedly disrupts autoregulation
- Nitric oxide, not important
- TGF

- Chloride in macula densa
- Blocked by furosemide
- Group affect of nephrons

- Ang 2 sensitizes
- Adenosine mediates
- Function of TGF
- 90% of filtrate is reabsobed in PT and LOH
- 10% is reabsobed dismally
- Need to control the amount of fluid delivered distally to prevent overwhelming the resorptive capacity of the distal nephron
- Talks about acute renal success without naming it (but did reference it)
- Mentions glucosuria blunts TGF. Hmmm...
- Neurohormonal influences

- Volume changes in ang2, sympathetic NS
- Role of PGE
- Interesting discussion of change of the nephrons perfumed with volume depletion, shifting of blood from outer coretex to inner medullary cortical gloms with their long loops
- Dopamine and ANP both increased with volume up
- Dopamine causes vasodilation of afferent and efferent arteriole
- ANP causes afferent vasodilation and efferent vasodilation constriction, increasing GFR without affecting RPF
- Glomerular hemodynamics and renal failure
- Decreased glomerular mass results in hyperfiltration of remaining gloms
- Mediated through afferent vasodilation
JC talks about this classic study in critical care: High vs. Low blood pressure target in Septic Shock. https://www.nejm.org/doi/pdf/10.1056/NEJMoa1312173
In this multi-center open label trial of 776 patients randomized to either a MAP of 65-70 or 80-85 with the primary endpoint of mortality. There was no difference in mortality at 28 days between the two groups (but a small difference in AKI in the patients who had chronic HTN- in the higher BP target, there was a decrease in need for RRT; there was also a higher incidence of afib in the high target group overall).
- Results in compensation and stable GFR in short term, long term maladaptive
- Reason for ACEi
- Clinical Evaluation of Renal Circulation
- Concept of clearance and measurement of GFR
- GFR as an index of functioning renal mass
- Had a patient today s/p nephrotomy, 72 years old, Cr0.9!
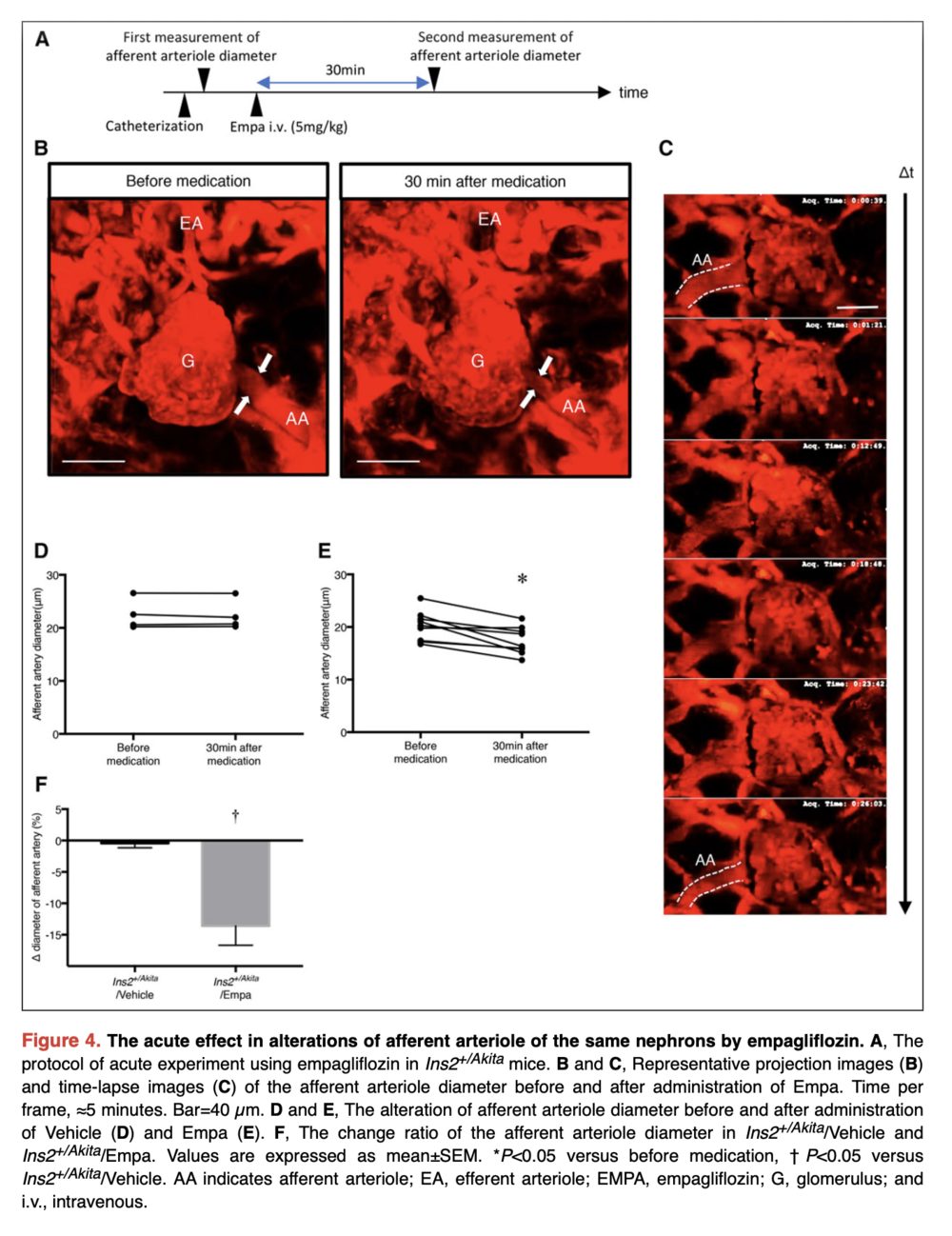
Melanie referred to this article in Circulation which demonstrates that SGLT2 inhibitors do decrease single nephron GFR (in mice) and that this is related to a decrease in the afferent arteriole diameter and then they show that this is related to a local increase in adenosine.
Kidokoro K, Cherney DZI et al. Evaluation of glomerular hemodynamic function by empagliflozin in diabetic mice using in vivo imaging Circulation 140 (4) 2019
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.118.037418
- Fall in GFR earlier and only sign of renal disease
- Serial monitoring is used to assess severity and follow the course of disease
- GFR is useful for dosing drugs
- How to measure GFR

- Consider fructose polysaccharide inulin (love the parenthetical, not insulin)
- Inulin filtered = inulin excreted
- Filtered inulin = plasma inulin concentration x GFR
- Inulin excreted = urine concentration x urine volume
- Use Alber a to get GFR = [Urine]insulin x urine volume / [plasma]inulin
- GFR = inulin clearance
- There is not an available assay for inulin
- Creatinine clearance
- Freely filtered
- Not reanbsorbed
- Not metabolized
- Small amount excreted
- CrCl exceeds GFR by 10-20%
Roger says the SGLT2 inhibitor story is about the afferent arteriole and he thought it reminded him of the MDRD study and the concept that the lower protein intake would be protective and delay the progression of CKD.
The concept was that low protein diets would decrease glomerular pressure by decreasing the intake of amino acids that lead to arteriolar vasodilation and increased GFR. Klaur S, Levey AS et al. The effects of Dietary Protein Restirciton and blood-pressure control on the progression of chronic renal disease. NEJM 1994 330:877-884.
https://www.nejm.org/doi/full/10.1056/nejm199403313301301
- Compensated for by noncreatinine chromogens (acetone proteins, as Orbi acid, pyruvate) that over estimate Cr by 10-20%
- Cr Cl = [Urine]cr x urine volume / [Plasma]cr
- Two major limitations
- Incomplete collections
- 20-25 mg/kg in adult men
- 15-20 mg/kg in adult women
The term “Acute renal success” comes from
Thurau K and Boylan JW. Acute renal success. The unexpected logic of oliguria in acute renal failure. Am J Med 1976 61(3): 3038-15.
- Falls by 50% from age 50 to 90 to 10 mg/kg
- Increased tubular secretion with decreased kidney function

- GFR of 40-80 cr secretion may account for as much as 35% of creatinine excretion
- In some cases CrCl can exceed GFR by a factor of 2
- Give cimetidine 1200 mg!
- It is important to appreciate however that exact knowledge of GFR is not required. More important to know if GFR is changing
- Why is radio labeling the solution DTPA and iothalamate?
- Talks about the reality of progressive disease despite stable GFR and CrCl
- On to plasma Cr and GFR
If you think placing dialysis lines is too easy, here is a wonderful review of micropuncture technique in the kidneys by Volker Vallon.
Micropuncturing the Nephron. Pflugers Arch 2009 458(1): 189-201. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2954491/
- Creatinine excretion = creatinine production (and this is constant)
- Creatinine excretion = [Cr] x GFR = constant
- If GFR falls in half, creatinine excretion will fall in half, while creatinine production remains the same, so creatinine will rise and rise until [Cr] x GFR = creatinine production and then it will level off.
- Changes in creatinine load
- High protein diet can increase it
- Vegetarian diet can decrease it
JC brought up studies on fenoldopam, of which there are many. This is one such study in patients undergoing cardiac surgery.
JAMA 2014 Bove T et al. Effect of fenoldopam on use of renal replacement therapy among patients with acute kidney injury after cardiac surgery: a randomized clinical trial https://pubmed.ncbi.nlm.nih.gov/25265449/
- Cooked meat can increase Cr by 1 mg/dL
- Talks about need for steady state to assess GFR
- Talks about the curvilinear relationship
- Then he talks Cockcroft Gault
The one, the only: The Cockcroft Gault:
Prediction of creatinine clearance from serum creatinine. Nephron 16: 31–41, 1976 https://pubmed.ncbi.nlm.nih.gov/1244564/
- Cirrhosis masks kidney insufficiency, low meat intake, low BUN production
- Can someone explain what we are supposed to take from figure 2-12
- Stable Cr does not mean stable kidney disease
Roger describes the study design for the seminal paper on the use of ACE inhibitors to slow the decline in renal function in diabetic kidney disease (then called diabetic nephropathy) and the decision to use the doubling of the serum creatinine as an endpoint.
Lewis EJ The effect of Angiotensin-converting-enzyme inhibition on diabetic nephropathy NEJM 1993 https://www.nejm.org/doi/full/10.1056/NEJM199311113292004
- Ketoacidosis can raise the Cr 0.5 to 2.0mg/dL
- On to BUN
- Destination of amino acids produces ammonia
- We detoxify ammonia by converting to urea
- Increased with increased protein load
- Increased catabolism
Melanie mentioned an old study on ingestion of expired blood: Cohen TD. Induced azotemia in humans following massive protein and blood ingestion and the mechanism of azotemia in gastrointestinal hemorrhage.
AM J Med Sci 1956 https://pubmed.ncbi.nlm.nih.gov/13302213/
- Tetracycline causes decreased anabolism
- Trauma
- Steroids
- Urea excretion is variable and tied to hydration and FF
- Renal plasma flow and PAH
21 episoade
Manage episode 288581724 series 2867323
Content provided by joel topf and Channel Your Enthusiasm. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by joel topf and Channel Your Enthusiasm or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://ro.player.fm/legal.
The exciting conclusion to
Chapter Two: Renal Circulation and Glomerular Filtration Rate
- Determinants of GFR
- First step in making urine is separation of an ultrafiltrate
- Governed by starling forces
- Balance of hydraulic and osmotic forces
- GFR = LpS (P gc – P us - Osmotic Pressure Cap p)
- Normal GFR 95 in women, 120 in men
- Cap Hydrolic pressure remains constant
- glom cap Oncotic progressively rises
- Due to filtration of protein free fluid (protein concentration rises in the capillary)
- Filtration gradient begins at 13 mmHg and falls to zero after filtration of 20% or RPF!
- GFR is capped at 20% of RPF called filtration equilibrium
- So GFR is dependent on RPF, unless you can change glomerular hydraulic pressure
- Glomerular hydraulic pressure is controlled by balance of twin arteriole (afferent and efferent)
- Constriction of afferent arteriole reduces RPF, GFR, and glom pressure
- Dilation of afferent arteriole increases RPF, GFR, and glom pressure
- Constriction of the efferent arteriole increases Glom pressure, increasing GFR
- Besides glom hydrostatic pressure the other starlings forces are rarely relevant to changes in GFR
Letty says: referred to this NEJM review article later JC thought she was referring to something else -see #2- and then Roger referred to this again)
Normotensive Acute Renal Failure from Gary Abuelo in NEJM 2007. https://www.nejm.org/doi/10.1056/NEJMra064398 (note in this article, Dr. Abuelo acknowledges the newer terminology of the time, AKI rather than ARF but chooses not to embrace it). In figure 2, he highlights the classic examples of how autoregulation can be affected. In the table, additional examples are provided but all within the framework of alterations related to autoregulation and the interplay between the two resistance vessels.
- Regulation of GFR
- Autoregulation
- The ability to keep glomerular pressure constant over wide range of systemic arterial pressure
- When pressure < 70 autoregulation fails and GFR will fall with decreases in systemic pressure
- When pressure falls below 40-50 GFR ceases
- At least some of this autoregulation is mediated with Ang2. Giving ACEi markedly disrupts autoregulation
- Nitric oxide, not important
- TGF
- Chloride in macula densa
- Blocked by furosemide
- Group affect of nephrons
- Ang 2 sensitizes
- Adenosine mediates
- Function of TGF
- 90% of filtrate is reabsobed in PT and LOH
- 10% is reabsobed dismally
- Need to control the amount of fluid delivered distally to prevent overwhelming the resorptive capacity of the distal nephron
- Talks about acute renal success without naming it (but did reference it)
- Mentions glucosuria blunts TGF. Hmmm...
- Neurohormonal influences
- Volume changes in ang2, sympathetic NS
- Role of PGE
- Interesting discussion of change of the nephrons perfumed with volume depletion, shifting of blood from outer coretex to inner medullary cortical gloms with their long loops
- Dopamine and ANP both increased with volume up
- Dopamine causes vasodilation of afferent and efferent arteriole
- ANP causes afferent vasodilation and efferent vasodilation constriction, increasing GFR without affecting RPF
- Glomerular hemodynamics and renal failure
- Decreased glomerular mass results in hyperfiltration of remaining gloms
- Mediated through afferent vasodilation
JC talks about this classic study in critical care: High vs. Low blood pressure target in Septic Shock. https://www.nejm.org/doi/pdf/10.1056/NEJMoa1312173
In this multi-center open label trial of 776 patients randomized to either a MAP of 65-70 or 80-85 with the primary endpoint of mortality. There was no difference in mortality at 28 days between the two groups (but a small difference in AKI in the patients who had chronic HTN- in the higher BP target, there was a decrease in need for RRT; there was also a higher incidence of afib in the high target group overall).
- Results in compensation and stable GFR in short term, long term maladaptive
- Reason for ACEi
- Clinical Evaluation of Renal Circulation
- Concept of clearance and measurement of GFR
- GFR as an index of functioning renal mass
- Had a patient today s/p nephrotomy, 72 years old, Cr0.9!
Melanie referred to this article in Circulation which demonstrates that SGLT2 inhibitors do decrease single nephron GFR (in mice) and that this is related to a decrease in the afferent arteriole diameter and then they show that this is related to a local increase in adenosine.
Kidokoro K, Cherney DZI et al. Evaluation of glomerular hemodynamic function by empagliflozin in diabetic mice using in vivo imaging Circulation 140 (4) 2019
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.118.037418
- Fall in GFR earlier and only sign of renal disease
- Serial monitoring is used to assess severity and follow the course of disease
- GFR is useful for dosing drugs
- How to measure GFR
- Consider fructose polysaccharide inulin (love the parenthetical, not insulin)
- Inulin filtered = inulin excreted
- Filtered inulin = plasma inulin concentration x GFR
- Inulin excreted = urine concentration x urine volume
- Use Alber a to get GFR = [Urine]insulin x urine volume / [plasma]inulin
- GFR = inulin clearance
- There is not an available assay for inulin
- Creatinine clearance
- Freely filtered
- Not reanbsorbed
- Not metabolized
- Small amount excreted
- CrCl exceeds GFR by 10-20%
Roger says the SGLT2 inhibitor story is about the afferent arteriole and he thought it reminded him of the MDRD study and the concept that the lower protein intake would be protective and delay the progression of CKD.
The concept was that low protein diets would decrease glomerular pressure by decreasing the intake of amino acids that lead to arteriolar vasodilation and increased GFR. Klaur S, Levey AS et al. The effects of Dietary Protein Restirciton and blood-pressure control on the progression of chronic renal disease. NEJM 1994 330:877-884.
https://www.nejm.org/doi/full/10.1056/nejm199403313301301
- Compensated for by noncreatinine chromogens (acetone proteins, as Orbi acid, pyruvate) that over estimate Cr by 10-20%
- Cr Cl = [Urine]cr x urine volume / [Plasma]cr
- Two major limitations
- Incomplete collections
- 20-25 mg/kg in adult men
- 15-20 mg/kg in adult women
The term “Acute renal success” comes from
Thurau K and Boylan JW. Acute renal success. The unexpected logic of oliguria in acute renal failure. Am J Med 1976 61(3): 3038-15.
- Falls by 50% from age 50 to 90 to 10 mg/kg
- Increased tubular secretion with decreased kidney function
- GFR of 40-80 cr secretion may account for as much as 35% of creatinine excretion
- In some cases CrCl can exceed GFR by a factor of 2
- Give cimetidine 1200 mg!
- It is important to appreciate however that exact knowledge of GFR is not required. More important to know if GFR is changing
- Why is radio labeling the solution DTPA and iothalamate?
- Talks about the reality of progressive disease despite stable GFR and CrCl
- On to plasma Cr and GFR
If you think placing dialysis lines is too easy, here is a wonderful review of micropuncture technique in the kidneys by Volker Vallon.
Micropuncturing the Nephron. Pflugers Arch 2009 458(1): 189-201. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2954491/
- Creatinine excretion = creatinine production (and this is constant)
- Creatinine excretion = [Cr] x GFR = constant
- If GFR falls in half, creatinine excretion will fall in half, while creatinine production remains the same, so creatinine will rise and rise until [Cr] x GFR = creatinine production and then it will level off.
- Changes in creatinine load
- High protein diet can increase it
- Vegetarian diet can decrease it
JC brought up studies on fenoldopam, of which there are many. This is one such study in patients undergoing cardiac surgery.
JAMA 2014 Bove T et al. Effect of fenoldopam on use of renal replacement therapy among patients with acute kidney injury after cardiac surgery: a randomized clinical trial https://pubmed.ncbi.nlm.nih.gov/25265449/
- Cooked meat can increase Cr by 1 mg/dL
- Talks about need for steady state to assess GFR
- Talks about the curvilinear relationship
- Then he talks Cockcroft Gault
The one, the only: The Cockcroft Gault:
Prediction of creatinine clearance from serum creatinine. Nephron 16: 31–41, 1976 https://pubmed.ncbi.nlm.nih.gov/1244564/
- Cirrhosis masks kidney insufficiency, low meat intake, low BUN production
- Can someone explain what we are supposed to take from figure 2-12
- Stable Cr does not mean stable kidney disease
Roger describes the study design for the seminal paper on the use of ACE inhibitors to slow the decline in renal function in diabetic kidney disease (then called diabetic nephropathy) and the decision to use the doubling of the serum creatinine as an endpoint.
Lewis EJ The effect of Angiotensin-converting-enzyme inhibition on diabetic nephropathy NEJM 1993 https://www.nejm.org/doi/full/10.1056/NEJM199311113292004
- Ketoacidosis can raise the Cr 0.5 to 2.0mg/dL
- On to BUN
- Destination of amino acids produces ammonia
- We detoxify ammonia by converting to urea
- Increased with increased protein load
- Increased catabolism
Melanie mentioned an old study on ingestion of expired blood: Cohen TD. Induced azotemia in humans following massive protein and blood ingestion and the mechanism of azotemia in gastrointestinal hemorrhage.
AM J Med Sci 1956 https://pubmed.ncbi.nlm.nih.gov/13302213/
- Tetracycline causes decreased anabolism
- Trauma
- Steroids
- Urea excretion is variable and tied to hydration and FF
- Renal plasma flow and PAH
21 episoade
Toate episoadele
×Bun venit la Player FM!
Player FM scanează web-ul pentru podcast-uri de înaltă calitate pentru a vă putea bucura acum. Este cea mai bună aplicație pentru podcast și funcționează pe Android, iPhone și pe web. Înscrieți-vă pentru a sincroniza abonamentele pe toate dispozitivele.
Similar cu Channel Your Enthusiasm
The key to learning Korean is how easy it is to stay motivated to learn the language. At TalkToMeInKorean.com, we provide a systematic curriculum of easy-to-follow lessons, and a wide selection of self-study Korean-learning books!
…
continue reading
Interviews with mathematics education researchers about recent studies. Hosted by Samuel Otten, University of Missouri. www.mathedpodcast.com Produced by Fibre Studios
…
continue reading
PT Inquest is an online journal club. Hosted by Jason Tuori, Megan Graham, and Chris Juneau, the show looks at an article every week and discusses how it applies to current physical therapy practice.
…
continue reading
Seeking a healthier emotional life? It’s time to bring a trained psychologist and mental health expert along for the ride. Dr. Monica Johnson explains the why behind complex emotions, helps you form better relationships, and guides you down the path of self-understanding.
…
continue reading
From host Kevin Miller: When I was 7 years old and got out of line, my parents would give me an “attitude adjustment” and make me listen to motivational speakers like Zig Ziglar. I didn’t appreciate it at the time but the experience gave me awareness of how powerful our minds and outlook on life are. I went on to become a pro athlete, have 9 kids, start 17 businesses and become addicted to performance and production. Till I burnt out. Multiple times. That started a quest to not just pursue p ...
…
continue reading
The award-winning Curiosity Daily podcast from CuriosityDaily.com will help you get smarter about the world around you. In less than 10 minutes, you’ll get a unique mix of research-based life hacks, the latest science and technology news, and more. Nate Bonham and Calli Gade will help you learn about your mind and body, outer space and the depths of the sea, and how history shaped the world into what it is today.Head to discovery+ to stream even more science content, from Animal Planet to Sc ...
…
continue reading
Emergency Medicine Cases – Where the Experts Keep You in the Know. For show notes, quizzes, videos and more learning tools please visit emergencymedicinecases.com
…
continue reading
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
The London School of Economics and Political Science public events podcast series is a platform for thought, ideas and lively debate where you can hear from some of the world's leading thinkers. Listen to more than 200 new episodes every year.
…
continue reading
Culips English Podcast: Practical English Learning Made Fun Learn and Explore: Join Culips for an exciting English learning journey. Our podcast focuses on teaching English idioms, slang, and phrasal verbs through fun and engaging conversations. Each episode helps you master English for real-life situations. Unique Learning Experience: Culips stands out by blending language skills with cultural insights. Our diverse hosts make learning relatable, covering a variety of everyday topics. You’ll ...
…
continue reading
Player FM - Aplicație Podcast
Treceți offline cu aplicația Player FM !
Treceți offline cu aplicația Player FM !



